Benefits of NEWS2:
- Provides a single standardised early warning system across the UK for early detection of the acutely unwell patient
- Provides a standardised score to determine illness severity to support consistent clinical decision making and an appropriate clinical response
- Provides a vehicle for the adoption of a standardised scoring system throughout the acute hospital, not solely in the context of acute clinical deterioration but also for continuous monitoring of all patients (Track and Trigger)
- Ensures a standardised means of identifying and responding to patients with unanticipated acute deterioration in their clinical condition whilst in hospital
There are two main ways in which NEWS2 should be used:
1. To provide a continuous record of a patient's physiological status throughout the patient journey (Track)
and
2. To provide a standardised platform for the initial assessment of acute illness severity wherever that assessment occurs (Trigger)
1. To provide a continuous record of a patient's physiological status throughout the patient journey (Track)
and
2. To provide a standardised platform for the initial assessment of acute illness severity wherever that assessment occurs (Trigger)
Be aware that NEWS2 is designed for use in adults aged 16 years and above.
NEWS2 is not recommended for use in children or during pregnancy. Baseline physiological parameters differ in children and in pregnancy where the magnitude and character of the physiological response to acute illness also differ.
NEWS2 may be unreliable in patients with spinal cord injury (especially tetraplegia or high-level paraplegia), owing to functional disturbances of the autonomic nervous system. Use with caution.
NEWS2 is not recommended for use in children or during pregnancy. Baseline physiological parameters differ in children and in pregnancy where the magnitude and character of the physiological response to acute illness also differ.
NEWS2 may be unreliable in patients with spinal cord injury (especially tetraplegia or high-level paraplegia), owing to functional disturbances of the autonomic nervous system. Use with caution.
Step 1
Measure and record the score for each of the 6 physiological parameters.
Step 2
Add all the physiological parameter scores together (aggregate) to calculate the NEWS2 score.
AND
Check if the trigger threshold for a single parameter has been reached.
Step 3
Identify the correct clinical response to the trigger, in terms of:
Measure and record the score for each of the 6 physiological parameters.
Step 2
Add all the physiological parameter scores together (aggregate) to calculate the NEWS2 score.
AND
Check if the trigger threshold for a single parameter has been reached.
Step 3
Identify the correct clinical response to the trigger, in terms of:
- The urgency of response
- The clinical competencies of the responder(s)
- The frequency of clinical monitoring required
- The most appropriate clinical setting for ongoing care.
Here are the 6 physiological parameters.
1. Respiratory rate
An elevated respiratory rate is a powerful sign of acute illness and distress, in all patients. The respiratory rate may also be elevated as a consequence of generalised pain and distress, sepsis remote from the lungs, CNS disturbance and metabolic disturbances such as metabolic acidosis.
A reduced respiratory rate is an important indicator of CNS depression and narcosis.
2. Oxygen saturations
Scale 1
The existing SpO2 scoring system that would apply to the majority of patients.
The non-invasive measurement of oxygen saturation by pulse oximetry is routinely used in clinical assessment in the acute setting.
Scale 2
A dedicated SpO2 scoring system for patients with hypercapnic respiratory failure whose desired oxygen saturations are set at a lower level (88-92%), with the NEWS scoring system adjusted accordingly.
The new SpO2 scoring Scale 2 is for patients with a prescribed oxygen saturation requirement of 88-92% (eg in patients with hypercapnic respiratory failure). This should only be used in patients confirmed to have hypercapnic respiratory failure on blood gas analysis on either a prior, or their current, hospital admission.
The decision to use the new SpO2 scoring Scale 2 should be made by a competent clinical decisionmaker and should be recorded in the patient's clinical notes.
In all other circumstances, the regular NEWS SpO2 scoring scale (Scale 1) should be used.
For the avoidance of doubt, the SpO2 scoring scale not being used should be clearly crossed out across the chart.
Patients requiring supplemental oxygen are at greater clinical risk. Thus, the requirement for supplemental oxygen to maintain satisfactory oxygen saturations has been incorporated into the scoring system.
A weighting score of 2 should be added to the aggregate NEWS2 score for any patient requiring supplemental oxygen. The mode and rate of oxygen delivery are often poorly documented. Recording the rate of oxygen flow (L/min) without recording the mode of delivery or device does not define how much oxygen the patient is receiving.
1. Respiratory rate
An elevated respiratory rate is a powerful sign of acute illness and distress, in all patients. The respiratory rate may also be elevated as a consequence of generalised pain and distress, sepsis remote from the lungs, CNS disturbance and metabolic disturbances such as metabolic acidosis.
A reduced respiratory rate is an important indicator of CNS depression and narcosis.
2. Oxygen saturations
Scale 1
The existing SpO2 scoring system that would apply to the majority of patients.
The non-invasive measurement of oxygen saturation by pulse oximetry is routinely used in clinical assessment in the acute setting.
Scale 2
A dedicated SpO2 scoring system for patients with hypercapnic respiratory failure whose desired oxygen saturations are set at a lower level (88-92%), with the NEWS scoring system adjusted accordingly.
The new SpO2 scoring Scale 2 is for patients with a prescribed oxygen saturation requirement of 88-92% (eg in patients with hypercapnic respiratory failure). This should only be used in patients confirmed to have hypercapnic respiratory failure on blood gas analysis on either a prior, or their current, hospital admission.
The decision to use the new SpO2 scoring Scale 2 should be made by a competent clinical decisionmaker and should be recorded in the patient's clinical notes.
In all other circumstances, the regular NEWS SpO2 scoring scale (Scale 1) should be used.
For the avoidance of doubt, the SpO2 scoring scale not being used should be clearly crossed out across the chart.
Patients requiring supplemental oxygen are at greater clinical risk. Thus, the requirement for supplemental oxygen to maintain satisfactory oxygen saturations has been incorporated into the scoring system.
A weighting score of 2 should be added to the aggregate NEWS2 score for any patient requiring supplemental oxygen. The mode and rate of oxygen delivery are often poorly documented. Recording the rate of oxygen flow (L/min) without recording the mode of delivery or device does not define how much oxygen the patient is receiving.

|
The NEWS2 chart has been updated to allow clearer recording of whether the patient is breathing air or oxygen; the device being used, if any; and the rate of oxygen delivery. For the documentation of the oxygen delivery system, the device codes as recommended by the BTS should be used. |
3. Systolic blood pressure
Although an elevated blood pressure (hypertension) is an important risk factor for cardiovascular disease, it is a low or falling systolic blood pressure (hypotension) that is most significant in the context of assessing acute-illness severity.
4. Pulse rate
The measurement of heart rate is an important indicator of a patient's clinical condition.
5. Level of consciousness and new confusion
A change in the level of consciousness is an important indicator of acute-illness severity. The assessment is done in sequence and only one outcome is recorded. For example, if the patient responds to voice, it is not necessary to assess the response to pain.
Beyond the recording of level of consciousness using the AVPU scale, it is well recognised that the onset of acutely altered mentation, ie 'new confusion' (delirium), can be an important sign that a patient requires urgent assessment. New-onset confusion (any new reduction in the Glasgow Coma Scale or delirium would also fit this criterion) is a sign of potentially serious clinical deterioration in patients and especially those with confirmed or suspected sepsis. NEWS2 includes 'new confusion' as part of the assessment of consciousness, hence the term ACVPU rather than AVPU to reflect this change. New confusion scores 3 on the NEWS2 chart, indicating a code red (for a single score of 3), ie that the patient requires urgent assessment.
6. Temperature
Both pyrexia and hypothermia are included in the NEWS2 scoring system reflecting the fact that the extremes of temperature are sensitive markers of acute-illness severity and physiological disturbance.
Although an elevated blood pressure (hypertension) is an important risk factor for cardiovascular disease, it is a low or falling systolic blood pressure (hypotension) that is most significant in the context of assessing acute-illness severity.
- Hypotension may indicate circulatory compromise due to sepsis or volume depletion, cardiac failure or cardiac rhythm disturbance, CNS depression, hypoadrenalism and/or the effect of blood pressure lowering medications. It is important to note that some people have a naturally low systolic blood pressure (≤100 mmHg) and this might be suspected if the patient is well and all other physiological parameters are normal, or confirmed by reference to previous records of blood pressure.
- Hypertension is given less weighting in the context of acute-illness assessment. Severe hypertension, e.g. systolic blood pressure ≥ 200 mmHg, may occur as a consequence of pain or distress but it is important to consider whether the acute illness may also be a consequence of, or exacerbated by severe hypertension and take appropriate clinical action.
- Diastolic blood pressure does not form part of the scoring system for acute-illness severity because it does not add value in this context. However, diastolic blood pressure should be routinely recorded as it may be severely elevated and require treatment in some acute settings, i.e. accelerated hypertension
4. Pulse rate
The measurement of heart rate is an important indicator of a patient's clinical condition.
- Tachycardia may be indicative of circulatory compromise due to sepsis or volume depletion, cardiac failure, pyrexia, or pain and general distress. It may also be due to cardiac arrhythmia, metabolic disturbance, e.g. hyperthyroidism, or drug intoxication, e.g. sympathomimetics or anticholinergic drugs.
- Bradycardia is also an important physiological indicator. A low heart rate may be normal with physical conditioning, or as a consequence of medication, e.g. with beta-blockers. However, it may also be an important indicator of hypothermia, central nervous system (CNS) depression, hypothyroidism or heart block.
5. Level of consciousness and new confusion
A change in the level of consciousness is an important indicator of acute-illness severity. The assessment is done in sequence and only one outcome is recorded. For example, if the patient responds to voice, it is not necessary to assess the response to pain.
- Alert - A fully awake (although not necessarily orientated) patient. Such patients will have spontaneous opening of the eyes, will respond to voice (although may be confused) and will have motor function.
- New confusion - A patient may be alert but confused or disorientated. It is not always possible to determine whether the confusion is 'new' when a patient presents acutely ill. Such a presentation should always be considered to be 'new' until confirmed to be otherwise.
- Voice - The patient makes some kind of response when you talk to them, which could be in any of the three component measures of eyes, voice or motor? e.g. patient's eyes open on being asked, 'are you okay?'. The response could be as little as a grunt, moan, or slight movement of a limb when prompted by voice.
- Pain - The patient makes a response to a pain stimulus. A patient who is not alert and who has not responded to voice (hence having the test performed on them) is likely to exhibit only withdrawal from pain, or even involuntary flexion or extension of the limbs from the pain stimulus. The person undertaking the assessment should always exercise care and be suitably trained when using a pain stimulus as a method of assessing levels of consciousness.
- Unresponsive - This is also commonly referred to as 'unconscious'. This outcome is recorded if the patient does not give any eye, voice or motor response to voice or pain.
Beyond the recording of level of consciousness using the AVPU scale, it is well recognised that the onset of acutely altered mentation, ie 'new confusion' (delirium), can be an important sign that a patient requires urgent assessment. New-onset confusion (any new reduction in the Glasgow Coma Scale or delirium would also fit this criterion) is a sign of potentially serious clinical deterioration in patients and especially those with confirmed or suspected sepsis. NEWS2 includes 'new confusion' as part of the assessment of consciousness, hence the term ACVPU rather than AVPU to reflect this change. New confusion scores 3 on the NEWS2 chart, indicating a code red (for a single score of 3), ie that the patient requires urgent assessment.
6. Temperature
Both pyrexia and hypothermia are included in the NEWS2 scoring system reflecting the fact that the extremes of temperature are sensitive markers of acute-illness severity and physiological disturbance.
Calculating a Score
1. Measure and record the score for each of the 6 physiological parameters.
2. The scores for each parameter are then added together.
3. The weighting reflects the severity of the physiological disturbance.
Once a score is calculated, there are two mechanisms based on the NEWS which can trigger a clinical response:
1. Measure and record the score for each of the 6 physiological parameters.
2. The scores for each parameter are then added together.
3. The weighting reflects the severity of the physiological disturbance.
Once a score is calculated, there are two mechanisms based on the NEWS which can trigger a clinical response:
- An extreme variation in an individual physiological parameter, i.e. a score of 3 in any one parameter
- A total NEWS of 5 or more
|
Staff measure and record the six NEWS2 physiological parameters. These are weighted and added together to get the NEWS2 score.
For each parameter, a normal 'healthy' range is defined (see column 0). Measured values outside of this range (column 0) are allocated a score which is weighted according to the magnitude of deviation from the normal range. |

|
The scores for each parameter are then added together and if significant, trigger a clinical response.
|
The NEWS2 Observation Chart
Here is a shortened example of a NEWS2 chart. A patient's six physiological measurements are taken and recorded on this chart and the score added together. A graded clinical response will be determined by the total score. This will be covered in the next section. An example of a completed chart can be seen here. Note: We recommend that you write on the chart the actual readings for any observations with a score of 3 (red). |

|
NEWS2 and Sepsis
Sepsis should be considered in any patient with a known infection, signs or symptoms of infection, or in patients at high risk of infection, and a NEWS2 score of 5 or more - 'think sepsis'.
Sepsis should be considered in any patient with a known infection, signs or symptoms of infection, or in patients at high risk of infection, and a NEWS2 score of 5 or more - 'think sepsis'.

|
Patients with suspected infection and a NEWS2 score of 5 or more require urgent assessment and intervention by a clinical team competent in the management of sepsis and urgent transfer to hospital or transfer to a higher-dependency clinical area within hospitals, for ongoing clinical care.
If a score of 3 in a single parameter consider sepsis. |
Triggers and Thresholds
When a patient initially presents with an acute illness, or suffers an acute deterioration in their clinical condition, the NEWS2 will help determine urgency and scale of the clinical response required.
This has three key elements:
When a patient initially presents with an acute illness, or suffers an acute deterioration in their clinical condition, the NEWS2 will help determine urgency and scale of the clinical response required.
This has three key elements:
- The urgency of response;
- The seniority and clinical competencies of clinical staff required to attend to the patient;
- The setting in which the ongoing clinical care should be delivered.
- Low score group
- Low-medium score group
- Medium score group
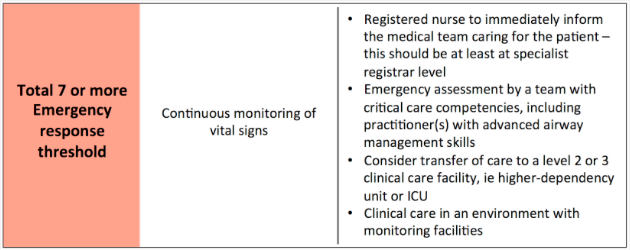
- High score group